Transforming Virtual Observation Through Clinician‑Centered UX Design
Collette Health needed to scale virtual observation safely in the middle of a national nursing shortage. I led a human‑factors redesign of the observation experience—grounded in ergonomics, central/peripheral vision research, and clinical co‑design—that reduced observer fatigue, increased clinical confidence, and enabled hospitals to safely expand from a 10:1 to a 12:1 patient‑to‑observer ratio. The work improved patient safety, reduced falls, and strengthened program adoption across hundreds of hospitals.
The Problem
Hospitals were facing a decades‑long nursing shortage, rising burnout, and increasing demand for patient observation. Traditional 1:1 sitters strained budgets and staffing, and early virtual observation systems were visually overwhelming and cognitively fatiguing. Observers struggled to maintain situational awareness across many video feeds, limiting program scalability and undermining clinical trust.
Clinicians reported:
Excessive head and eye movement to monitor multiple patients
Difficulty maintaining awareness across all feeds
Fatigue during long shifts
Stress from interfaces not aligned with clinical workflows
Without a UX foundation that supported long‑duration vigilance, hospitals couldn’t safely scale virtual observation.
Constraints
The redesign had to solve several intertwined challenges:
Human vision limits — Observers needed to see twelve patients at once without strain.
Ergonomics — The system had to fit the worker, not force adaptation.
Safety‑critical workflows — Observers needed rapid access to alarms, communication, and escalation.
Cognitive load — The interface had to support long shifts without degrading performance.
Scalability — Hospitals needed to safely move from 10:1 to 12:1 observation ratios.
These constraints made the work less about UI and more about human‑factors engineering.
Approach
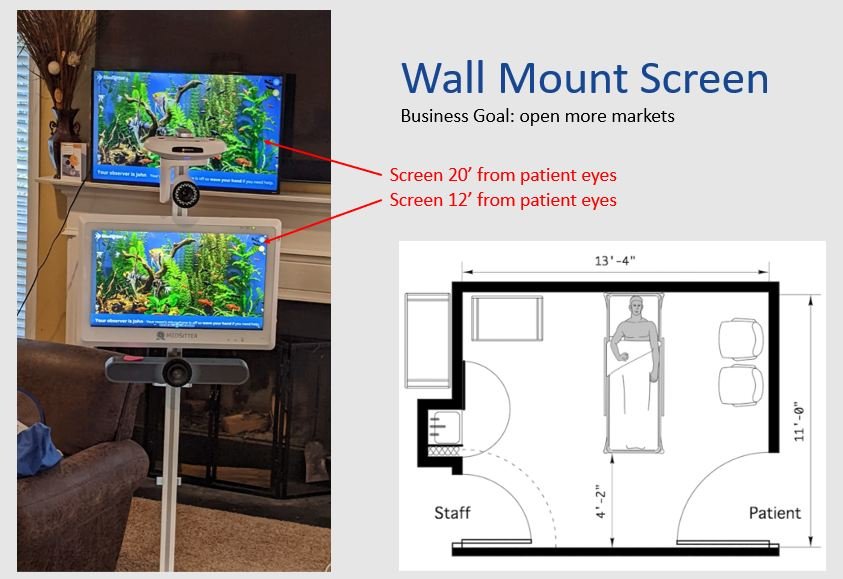
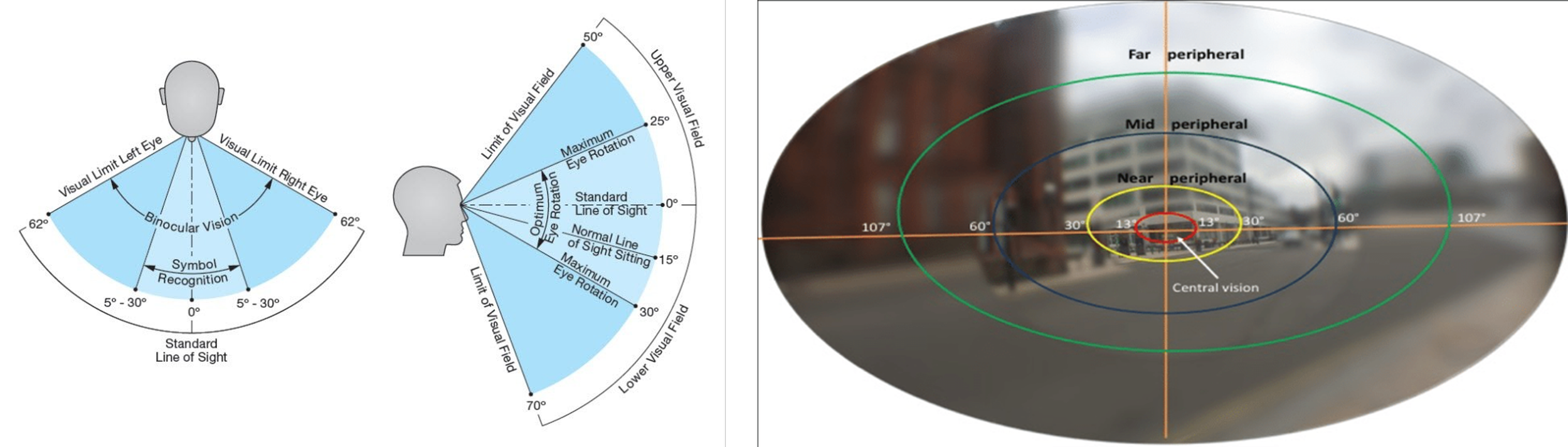
Ergonomics‑Driven Screen Architecture
I led research into central vs. peripheral vision to determine the optimal monitor size and layout. A 32‑inch display maximized edge‑to‑edge visibility without forcing head movement, enabling observers to see all twelve patients simultaneously.
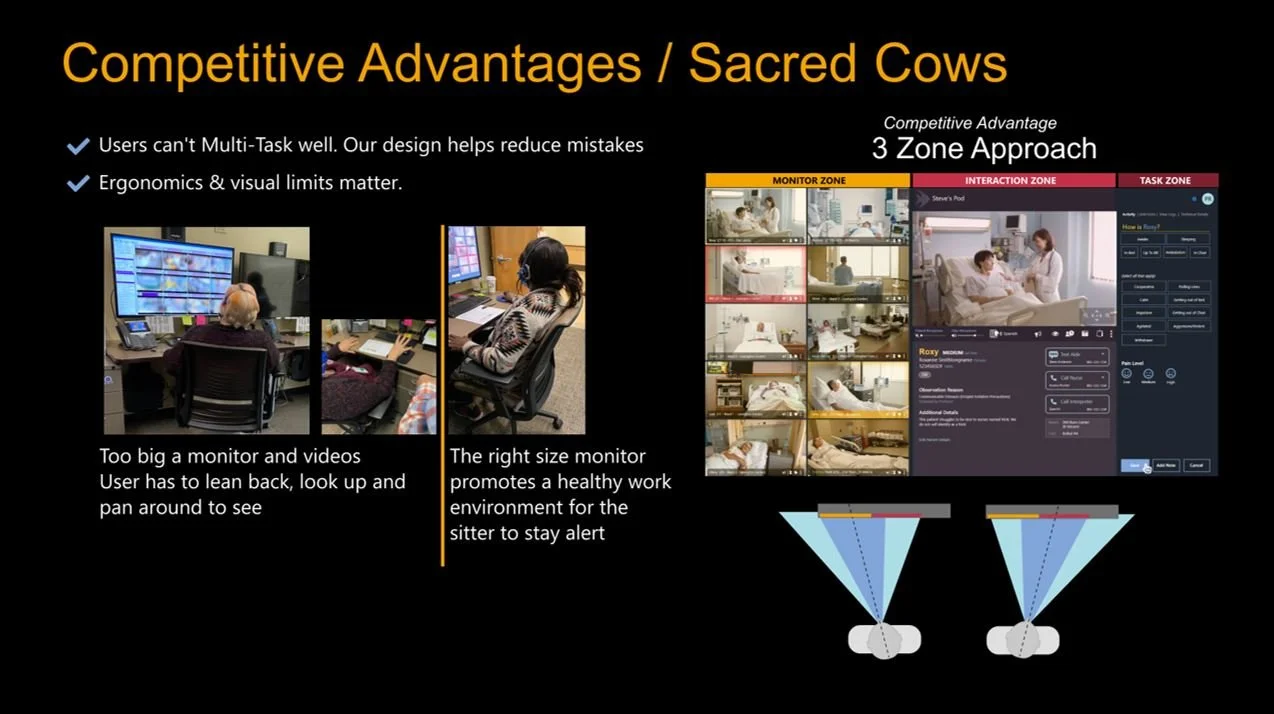
This informed a dual‑zone layout:
Interaction Zone for active engagement
Monitoring Zone for twelve peripheral feeds
Video Sizing Based on Real‑World Behavior
We validated feed sizes by studying how people naturally consume video. The redesigned feeds were more than 330% larger than typical vertical mobile video, ensuring clinical clarity without overwhelming the observer.
Reducing Fatigue Through Human‑Centered Interaction
I redesigned workflows to minimize motion and cognitive load:
Clear visual hierarchy
One‑click alarms and communication
Night‑vision and low‑light optimizations
Simplified interactions requiring no training
Clinical Co‑Design
RNs and CCRNs shaped alarm placement, workflow sequencing, and visual prioritization. Their input ensured the system aligned with real clinical practice and built trust with frontline team.

Outcomes
Expanded Observer Capacity
A safe increase from 10:1 to 12:1 patient‑to‑observer ratios—boosting capacity by 20% without adding staff.
Improved Patient Safety
68% reduction in fall rates
83,678 falls avoided
Improved HCAHPS scores across five domains
Reduced Fatigue and Higher Clinical Confidence
Observers could maintain situational awareness without strain, improving vigilance and reducing burnout.
Significant Labor Cost Savings
Hospitals achieved 10:1 labor cost savings by replacing 1:1 sitters with a scalable virtual observation model.
Stronger Program Adoption
Because the system required no training and reduced fatigue, clinicians trusted it—and used it—more consistently.
Result - By grounding the redesign in ergonomics, human‑vision science, and clinical workflow realities, we transformed virtual observation into a safer, more scalable, and more clinician‑friendly experience. The work improved patient safety, reduced observer fatigue, and enabled hospitals to expand their programs without adding staff—strengthening Collette Health’s position as the most trusted virtual observation platform in the market.
Citations
1. “Where Did All the Nurses Go?” Nursing, History, and Health Care, University of Pennsylvania's School of Nursing, https://www.nursing.upenn.edu/nhhc/workforce-issues/where-did-all-the-nurses-go. 2. “STUDY: 34% of Nurses Plan to Leave Their Current Role by the End of 2022.” Incredible Health, Incredible Health, 16 Mar. 2022, https://www.incrediblehealth.com/wp-content/uploads/2022/03/IHCOVID-19-2022-Summary-1.pdf. (no longer available)3. Valdez, Bart. “The Crisis in Healthcare Staffing.” Medical Economics, Medical Economics, 4 Feb. 2022, https://www.medicaleconomics.com/view/the-crisis-in-healthcare-staffing. 4. “STUDY: 34% of Nurses Plan to Leave Their Current Role by the End of 2022.” Incredible Health, Incredible Health, 16 Mar. 2022, https://www.incrediblehealth.com/wp-content/uploads/2022/03/IHCOVID-19-2022-Summary-1.pdf. (no longer available)5. Gangadharan, Prayag. “The Importance of User Experience Design.” UX Planet, UX Planet, 4 Aug. 2020, https://uxplanet.org/the-importance-of-user-experience-design-988faf6ddca2. 6. Gube, Jacob, et al. “What Is User Experience Design? Overview, Tools And Resources.” Smashing Magazine, Smashing Magazine, 5 Oct. 2010, https://www.smashingmagazine.com/2010/10/what-isuser-experience-design-overview-tools-and-resources/. (no longer available)7. “Ergonomics.” Environment, Health and Safety, University of North Carolina at Chapel Hill, 21 Mar. 2022, https://ehs.unc.edu/workplace-safety/ergonomics/. 8. Lipner, Maxine. “Understanding Central Vision.” Verywell Health, Verywell Health, 6 Dec. 2021, https://www.verywellhealth.com/central-vision-5209526. 9. Elizabeth Yuko, PhD. “What Is Peripheral Vision?” Verywell Health, Verywell Health, 1 Nov. 2021, https://www.verywellhealth.com/peripheral-vision-5097416. 10. Andres, Josh & Schraefel, Nathan & Semertzidis, & Dwivedi, Brahmi & Kulwe, Yutika & von Kaenel, Juerg & Mueller, Florian. (2020). Introducing Peripheral Awareness as a Neurological State for HumanComputer Integration. 10.1145/3313831.3376128.